Anorectal malformation, commonly known as imperforate anus, encompasses a range of conditions where individuals lack a normal anal opening. Instead, a fistulous tract opens onto the perineum, typically anterior to the anal muscle complex or into nearby anatomical structures. In males, the tract may connect to the urinary system, while in females, it may extend towards gynecologic structures. This condition requires careful evaluation and tailored surgical interventions to address the specific anatomical variations.
Anorectal Malformation in Male
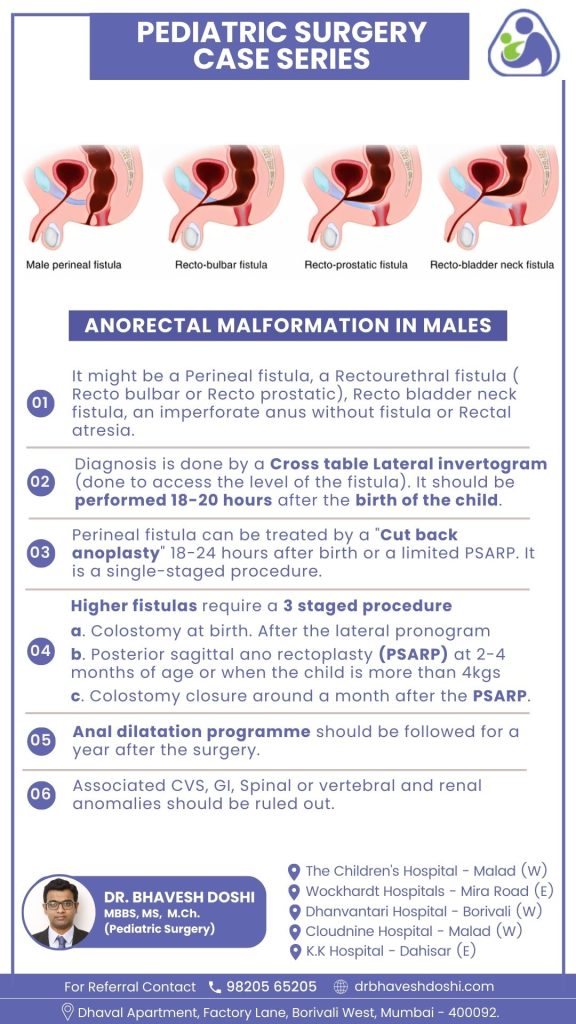
Types of Anorectal Malformations:
- Perineal Fistula: Diagnosed through a Cross-table Lateral Invertogram. Treatment includes “Cut back anoplasty” or limited Posterior Sagittal Ano Rectoplasty (PSARP) within 18-24 hours after birth.
- Rectourethral Fistula: Identified through diagnostic procedures, with the treatment approach varying based on specific anatomy, often involving a staged procedure.
- Recto Bladder Neck Fistula: Diagnosed through diagnostic assessments, and management may require a staged procedure.
- Imperforate Anus without Fistula or Rectal Atresia: Diagnosis involves a Cross-table Lateral Invertogram, and treatment depends on the specific condition, often employing a staged approach.
Diagnostic Procedure:
- Cross-table Lateral Invertogram performed 18-20 hours after birth to assess the level of the fistula.
Treatment Approaches:
- Perineal Fistula: Options include “Cut back anoplasty” or limited PSARP within 18-24 hours after birth.
- Higher Fistulas (Rectourethral, Recto Bladder Neck, Imperforate Anus without Fistula or Rectal Atresia):
Staged procedure:
a. Colostomy at birth.
b. PSARP at 2-4 months of age or when the child is more than 4 kgs.
c. Colostomy closure approximately a month after PSARP.
Postoperative Care:
- Anal dilatation program recommended for a year after surgery.
Associated Anomalies:
- Rule out associated anomalies in cardiovascular, gastrointestinal, spinal or vertebral, and renal systems.
Anorectal malformations in males require a comprehensive approach for diagnosis and treatment, with considerations for specific types, staged procedures, postoperative care, and assessment of associated anomalies ensuring a holistic management strategy.
Anorectal Malformations in Female
Types of Anorectal Malformations:
- Vestibular Fistula: Common in females, characterized by a small opening at the posterior fourchette of the vestibule. Diagnosis involves Cross-table Lateral Pronogram.
- Perineal Fistula: Identified through diagnostic assessments. Treatment options include single-staged Primary PSARP or PSARP with colostomy.
- Persistent Cloaca: Diagnosis involves evaluating the common channel length, with treatment considerations based on the channel size.
- Imperforate Anus without Fistula or Rectal Atresia: Diagnosis includes Cross-table Lateral Pronogram, and treatment options may involve staged procedures.
Diagnostic Procedure:
- Cross-table Lateral Pronogram performed 18-20 hours after birth to assess the level of the fistula.
Treatment Approaches:
- Vestibular Fistula: Rectal washes recommended until the child reaches 4 kgs or 2-3 months of age.
- Perineal Fistula: Options include single-staged Primary PSARP or PSARP with colostomy.
Postoperative Care:
- Anal dilatation program advised for 1 year after the procedure.
Outcome and Continence:
- Generally, females exhibit good results post the procedure, with continence being a positive outcome.
Anorectal malformations in females involve specific considerations such as Vestibular Fistula, which requires tailored diagnostic procedures and treatment approaches. Early diagnosis, staged procedures, and postoperative care contribute to favorable outcomes, emphasizing continence and overall well-being.